

08 März White Paper: How inhaler technique influences drug approval & de-risking clinical development programs
What if your inhaled active substance could make a decisive difference, but the inhaler device is used incorrectly by patients?
-
Poor inhalation technique is expensive
Inhaled drug delivery is the cornerstone of the treatment of respiratory diseases, such as chronic obstructive airway diseases like asthma and chronic obstructive pulmonary disease (COPD), but also numerous rare diseases, e.g. pulmonary hypertension or cystic fibrosis. After tablets, inhaled therapies are the most commonly prescribed form of medication worldwide (6). Despite the widespread availability of effective inhaled therapies for asthma and COPD, disease control is often suboptimal (1) due to poor adherence and/or inhalation errors.
The correct of use of Inhaler devices such as Dry powder Inhalers (DPIs) or Metered Dose Inhalers (MDI) is essential for the effective treatment of respiratory diseases, only then will a sufficient medication dose reach the lungs. Unfortunately, using inhalers is not easy and patients often struggle with them. Numerous studies have shown that patient inhaler device handling errors are frequent and result in poorly controlled or uncontrolled respiratory disease (1,2,3).
In short, while inhaled therapies represent a very effective approach to treat a variety of diseases, these same therapies have inherent adherence, device and dose delivery challenges. These affect patients but also increase the clinical development and launch risks for pharmaceutical companies as therapy success ultimately depends on good, reproducible drug delivery.
The best inhaled drugs will only be most effective if delivered correctly.
If the inhalative substance developed at great expense does not reach the lungs because of incorrect usage of inhalers, clinical effects may not be seen, clinical studies may not produce the expected and achievable results, or they may even fail. This risk is not theoretical, as you will see when we look at the risks and difficulties of inhaled therapy. Furthermore, this risk is well described in numerous studies and should be mitigated.
What if there was a new way to improve inhaler technique with patients?
Find out more about Kata®, a smartphone-based digital adherence solution, specifically designed for inhaled therapies, that analyzes and coaches patients’ inhalation techniques in real time, reduces dose- delivery risks, ultimately improving disease outcomes.
- Inhalation therapy – a complex mode of application/ administration
Medication adherence, i.e., the degree to which use of medication by the patient corresponds with the prescribed regimen, is a major challenge in chronic illness (4). Adherence is a big issue in chronic respiratory conditions such as asthma and COPD because patients feel overwhelmed by or insecure with the complexity of the inhalation procedure. So called “effective adherence” is only achieved when the patient takes the correct medication at the correct time, and also uses the inhaler in the correct way (5,6).
Correct inhalation technique is the key to effective delivery of high and reproducible doses of an aerosolized drug to the lungs. But correct inhalation is much more complex than swallowing a pill. Many steps must be followed in the correct order and execution.
- Preparing the inhaler (i.e., removing the mouthpiece cover, preparing a dose of the drug, shaking the inhaler)
- Full exhalation
- Enclosing the mouthpiece
- Correct inhalation and commonly actuation of the inhaler at the right time
- Holding the breath
Studies show that inhaled therapy is prone to errors (1, 2). Incorrect dose preparation, insufficient exhalation before inhalation, insufficient inspiratory effort and speed (depending on the inhaler type), failure to remove the cap, exhaling into the device before inhalation, problems coordinating inhaling and pressing at the same time, not holding the breath at all or long enough after the inhalation are some typical errors that occur regularly (1).
Inhaler users usually make a combination of errors during a single inhalation. Factors such as older age, lower levels of education and a lack of instruction from healthcare providers contribute to inhaler misuse, but errors are widely distributed among all inhaler users.
Windisch et al.(7) reported that only 4.4 % of the 159 recruited patients did not make multiple inhalation errors, while 95.6 % made multiple handling errors when using inhalers as they would at home.
Up to 90 % of patients do not use their prescribed inhaler correctly (1, 8, 10).
Another factor is the large number of different inhalers on the market. The three main categories of inhalers are metered-dose inhalers (MDIs), dry- powder inhalers (DPIs), and soft-mist inhalers. Currently, more than 160 different combination preparations with MDI and DPI inhalers are approved. Each Inhaler type differs in its application which adds a further level of complexity for patients.
Finally, a major challenge with inhaled therapies and the use of inhaler devices is, that while the inhalation training is either done at the physician’s office or via a video, patients then inhale on a chronic basis, at home, without supervision or the possibility of an intervention.
They certainly can record if they have inhaled their medication or not, but might not know whether they have done it well.
Quality of adherence is thus a significant challenge both in clinical practice as well as clinical development settings.
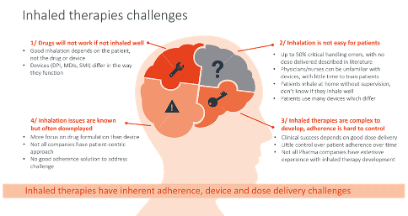
Figure 1: Overview of challenges in inhaled therapy.
2.1 Consequences of poor inhalation quality for patients and disease management
Incorrect use of inhalers has severe consequences:
- The delivery of the active component is partially or completely reduced: Only correct inhalation procedures ensure delivery and distribution to the entire lungs.
- Reduced efficacy of the active component: Depending on the type and combination of errors, either little efficacy can be expected or the application is useless.

Figure 2: Schematic diagram of the effects of wrong versus right inhaler technique.
- Reduced disease control: As shown in a number of studies, inhaler errors lead to worsened control of respiratory disease (1, 2, 7, Figure 2)
- Reduced adherence to treatment or study protocol: Patient adherence is not solely a function of treatment efficacy. However, little or no improvement in symptoms further reduces adherence.
- Increase of exacerbations: Poorly controlled asthma or COPD increases the risk of exacerbations. Price et al (2) found associations between certain inhaler errors and an increased risk of exacerbations.

Figure 3: Misuse of pressurized metered dose inhalers is directly linked to decreased asthma stability: frequency distribution of the number of errors or omissions in inhalation technique (left axis; striped bars) and relationship between this number and the Asthma Instability Score (AIS; mean ± SEM, right axis; grey bars). Adapted from 9.
The negative impact of ineffective inhalation on patients is important to consider. It reduces confidence in inhaled therapies. Patients who don’t experience an improvement or stabilization of their symptoms will stop using inhalers, which has a negative impact on clinical outcomes. Moreover, many physicians assume that inhaled drugs are often ineffective and either do not prescribe them or do not participate in clinical trials. Thus, improving inhalation technique remains a key challenge for chronic respiratory diseases.
2.2 Consequences of poor inhalation for pharmaceutical companies and clinical trials
As shown before, inhalation therapies are prone to error. This is not only a problem for the care of individual patients. It is even more of an unpredictable risk for pharmaceutical companies and their clinical trials. Research and development of new drugs is costly and always involves risks. However, unnecessary obstacles should be avoided.
Clinical trials that investigate the efficacy of an inhaled product have the added challenge that subject adherence not only relies on taking the investigational product as prescribed, but also on inhalation technique (i.e., “effective adherence”).
Usually, inhaler training takes place at the beginning of a trial if there is any training at all. Analyses show that 50 % of patients never receive inhaler training (10, 11, 12).
Depending on the study design, patients who already have experience with inhalers and those with no previous experience can take part. While novice inhaler users, even with good training, can be overwhelmed by the complex multi-step process and make mistakes when using the inhaler at home, confusion among experienced inhaler users is caused by the different requirements when using different inhaler models/types.
More importantly, while inhalation training is a good initial step, the ability to coach and intervene to ensure consistent quality of inhalation becomes much more relevant in clinical trials investigating the efficacy of an inhaled investigational product.
Subject non-compliance, defined not only quantitatively but also qualitatively is a common problem in clinical trials with inhaled drugs and can have a significant impact on the outcomes (13).
This common problem of suboptimal inhaler technique has significant consequences for clinical trials:
- Safety profile: The route of administration may play a role in the safety of a compound. Data on the safety profile could be falsified by incorrect
- Dosage: Incorrect inhalation reduces the dose of medication reaching the lungs resulting in reduced effects of the drug and less improvement of symptoms. It may also simulate lower efficacy, so that the dosage for study participants is increased to achieve the desired Patients using the inhaler correctly will receive too high doses. The issue here is that unless you can measure the actual inhalation quality, you have no way to assess whether the dosage was correct or not, until the end of the study or the next visit, which is too late.
- Side effects: Less symptom improvement leads to an unfavorable ratio of effect to side effect, followed by low adherence and increased dropout
- Greater study effort: If inhalation is incorrect, the effect is likely to be smaller than if the drug is used optimally. Therefore, more patients need to be included in clinical trials in order to demonstrate a significant improvement. Alternatively, additional clinical trials may be needed, with all the associated costs.
- Delayed or rejected drug approval: The increased study effort and lower benefit compared to standard care or placebo may delay the drug approval process, restrict the indication or prevent approval altogether.
Each of these issues significantly increases the cost of the entire clinical trial and regulatory process.
The key to all of the above-mentioned consequences, however, is poor therapy adherence due to frequent, well documented, significant and often under-appreciated handling errors of inhalers.
Until now there was no good solution to address this problem. For the first time real-time coaching and monitoring of patients’ inhalation is possible.
The vicious circle can be broken. De-risk your clinical development program now. By mitigating inhalation errors with real-time intervention and coaching.
3. Improving inhalation therapy through correct and simple training
Looking at the list of common errors in inhalation therapy (page 3), it might seem that there is no end in sight to improving the situation. Fortunately, this is not the case.
It all starts with teaching proper inhalation technique and continues with keeping patients motivated to keep up the therapy regime.
Inhalation training is currently provided by study personnel or prescribing Healthcare Providers (HCPs) primarily. The problem is that this kind of coaching only takes place during one or few visits at the beginning of a therapy or study. When study participants then use the inhaler at home, they are not monitored and inhalation errors can creep in again. Without supervision, patients are also not aware of whether they are inhaling correctly or not.
This is where an innovative approach comes in to improve the quality of inhalation and significantly reduce inhalation errors (7).
Meet Kata®!
Receiving coaching, in real-time, on how to use the inhaler correctly and how to better benefit from the medication is very important for patient adherence. However, as inhaling is a greater effort, it is also important to remind and motivate patients to use their inhaler correctly. Kata® includes all of these features.
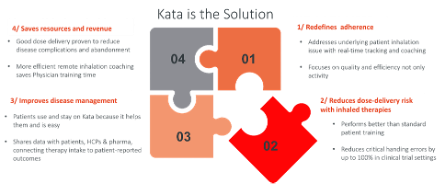
Figure 4: Using Kata® increases inhalation quality and improves disease management.
-
Kata® – the smartphone-based inhalation coach
Kata® is a digital AI based app that uses any smartphone’s audio and video sensors to measure inhalation quality and correct dose delivery to the lungs. The app provides real-time inhalation coaching for almost any inhaler on the market. The combination of artificial intelligence, machine learning, computer animation and augmented reality achieves a revolutionary and patient-centric improvement in the delivery of inhaled therapies. It redefines patient adherence for inhaled therapies from a quantitative measure to a much needed qualitative one.
4.1 How does Kata® work?
Using Kata® is simple. You only need your smartphone and the Kata® app. No other hardware is required. The app guides you through the entire inhalation process.
- Preparation: Once the app is installed, the first step is to enter your inhaled medication plan in the app, that is, which inhaler(s) do you use, at what time, etc. Once this plan is in the app, you are all set to us the Kata inhalation coach to support your
- Complete your inhalation together with the Kata inhalation coach: Simply select the next inhalation in your Kata medication plan and place your phone in front of This way, the inhalation coach guides you step by step through your inhalation.
- Inhalation Scoring and analysis: While you complete your inhalation with the Kata coach, the Kata algorithms use the camera and microphone signals of the smartphone to recognize and evaluate your inhalation, which is how effective the inhalation was in each phase (preparing the inhaler, exhalation, inhalation, holding the breath, exhalation).
- Feedback to the user: Once you have completed your inhalation, you will receive graphical and textual feedback on the inhalation process based on the real-time AI evaluation of your inhalation.
- Reminders: Once you have entered your personal medication plan in the app, Kata will also remind you of each inhalation so that you never forget to inhale.
- Patient motivation: Several in-app-applications further support patient adherence and motivation
4.2 Effects of Kata® usage on inhalation efficacy and adherence
- The advantages of such an easy-to-use application are obvious:
- Patients can use the Kata coach to guide their inhalations on a daily basis and receive personalized and direct feedback to improve their inhalation technique.
- Patients receive reminders to inhale, to make sure they do not forget to inhale.
- Handling errors are reduced by 95 % (14).
- Critical handling errors that result in a complete loss of inhalation effort are reduced by 100 % (14).
- Further remote patient monitoring features support regular inhalation and motivate patients to stick to their treatment regime (Chapter 5.1, page 8).

Figure 5: Inhaler error reduction by training by nurses and videos (industry standard) and Kata®. The use of Kata® reduces handling errors by 95 % and critical errors (no dose delivered when using inhaler) by 100 %. Data extracted from [1,7, 14].
5 How can Kata® be used in clinical trials?
The use of Kata® results in significant improvements for individual patients. In addition, we at Visionhealth are convinced that the use of Kata® in clinical trials helps to reduce risks of clinical research programs. Real-time coaching always improves the drug delivery and efficacy of the inhaled treatment. The comparability of study groups is improved, as study participants without inhalation experience are not disadvantaged compared to those with previous experience. In addition, patients with previous inhalation experience improve their inhalation quality.
Other features of the app help to motivate users and improve adherence to therapy – a problem that is particularly prevalent with inhalation therapies.
Besides the benefits of inhalation technique and patient adherence, the Kata app for clinical trials also offers means to monitor patients and to collect additional study data (e.g., questionnaires).
Kata® has been used in the following trials:

5.1 What Kata® can do for you
Are you planning a clinical trial and want to know how you can use Kata®?
There are a number of features that can be customized for each study according to the specific requirements.
AI inhalation trainer plus video recording
- Reliable drug-dose delivery to the lung during the trial
- Identification of irregularities that may have occurred and support for high risk patients
- Analysis of inhalation videos provides additional patient insights and usability data
- Minimization of overall study costs through efficient dose delivery
Digital Toolbox for your individual trial needs
- Video analysis of each inhalation and inhalation adherence graphs/reports
- Continuous patient monitoring, e.g., via patient compliance reports Safety parameters are continuously available with the possibility of fast data retrieval for analysis
- Implementation of any questionnaires to be completed during the trial Inhaled medications frequency/dosage
- Exercise frequency
- Patient reported outcomes like mood scores and comments Features can be added as needed
- Content, Layout and UIX can be customized to meet sponsor requirements (e. g. clinical protocol)
5.2 Patient data – security and handling
- The handling of patient data is of great importance to pharmaceutical companies and to VisionHealth.
- Kata is CE marked class IIa medical device according to Medical Device Regulation (MDR).
- Kata is listed as class I device according to the U.S. Food and Drug Administration (FDA).
- Kata® is fully compliant with GCP criteria. VisionHealth is ISO 13485 and ISO 27001 certified. Data handling is GDPR compliant
6. Kata® – game changer in inhalative clinical trials
Correct inhaler technique is essential for the effective treatment of asthma and COPD. Inhalation therapy is widely used around the world. However, many studies have shown that inhalation errors drastically reduce the effectiveness of inhaler therapy. And errors are very common. This can have huge impact on clinical trials and their results, and is a major risk for pharmaceutical companies.
The innovative Kata® app uses the smartphone’s camera and microphone to provide real-time inhalation coaching for many available inhalers. It is the first app to use artificial intelligence to measure inhalation quality and correct dose delivery to the lungs. Combined with computer animation and augmented reality, it brings a new dimension of improvement to inhalation management.
Correct inhalation technique can be a game changer in clinical trials. Correct inhalation ensures optimal drug delivery and the best clinical effects. It also reduces the costs and financial risks associated with inhalation trials.
Kata® also incorporates features to improve adherence. The application can be customized to meet the needs of your company or clinical trial.
Sources:
- Melani AS, Bonavia M, Cilenti V, Cinti C, Lodi M, Martucci P, Serra M, Scichilone N, Sestini P, Aliani M, Neri M; Gruppo Educazionale Associazione Italiana Pneumologi Inhaler mishandling remains common in real life and is associated with reduced disease control. Respir Med. 2011 Jun;105(6):930-8. doi: 10.1016/j.rmed.2011.01.005
- Price DB, Román-Rodríguez M, McQueen RB, Bosnic-Anticevich S, Carter V, Gruffydd-Jones K, Haughney J, Henrichsen S, Hutton C, Infantino A, Lavorini F, Law LM, Lisspers K, Papi A, Ryan D, Ställberg B, van der Molen T, Chrystyn Inhaler Errors in the CRITIKAL Study: Type, Frequency, and Association with Asthma Outcomes. J Allergy Clin Immunol Pract. 2017 Jul-Aug;5(4):1071-1081.e9. doi:
10.1016/j.jaip.2017.01.004
- Haughney J, Price D, Kaplan A, Chrystyn H, Horne R, May N, Moffat M, Versnel J, Shanahan ER, Hillyer EV, Tunsäter A, Bjermer Achieving asthma control in practice: understanding the reasons for poor control. Respir Med. 2008 Dec;102(12):1681-93. doi:
10.1016/j.rmed.2008.08.003
- World Health Adherence to long-term therapies: evidence for action. 2003. ISBN 9241545992. https://iris.who.int/handle/10665/42682 (accessed 21/02/2024)
- Braido F, Chrystyn H, Baiardini I, Bosnic-Anticevich S, van der Molen T, Dandurand RJ, Chisholm A, Carter V, Price D; Respiratory Effectiveness „Trying, But Failing“ – The Role of Inhaler Technique and Mode of Delivery in Respiratory Medication Adherence. J Allergy Clin Immunol Pract. 2016 Sep-Oct;4(5):823-32. doi: 10.1016/j.jaip.2016.03.002
- Pritchard JN, Nicholls Emerging technologies for electronic monitoring of adherence, inhaler competence, and true adherence. J Aerosol Med Pulm Drug Deliv. 2015 Apr;28(2):69-81. doi: 10.1089/jamp.2014.1163
- Windisch W, Schwarz SB, Magnet FS, Dreher M, Schmoor C, Storre JH, Knipel Using web-based videos to improve inhalation technique in COPD patients requiring hospitalization: A randomized controlled trial. PLoS One. 2018 Oct 16;13(10):e0201188. doi: 10.1371/journal.pone.0201188
- Adeloye D, Chua S, Lee C, Basquill C, Papana A, Theodoratou E, Nair H, Gasevic D, Sridhar D, Campbell H, Chan KY, Sheikh A, Rudan I; Global Health Epidemiology Reference Group (GHERG). Global and regional estimates of COPD prevalence: Systematic review and meta- J Glob Health. 2015 Dec;5(2):020415. doi: 10.7189/jogh.05.020415
- Giraud V, Roche Misuse of corticosteroid metered-dose inhaler is associated with decreased asthma stability. Eur Respir J. 2002 Feb;19(2):246-51. doi: 10.1183/09031936.02.00218402
- Lavorini F, Magnan A, Dubus JC, Voshaar T, Corbetta L, Broeders M, Dekhuijzen R, Sanchis J, Viejo JL, Barnes P, Corrigan C, Levy M, Crompton GK. Effect of incorrect use of dry powder inhalers on management of patients with asthma and COPD. Respir Med. 2008
Apr;102(4):593-604. doi: 10.1016/j.rmed.2007.11.003
- Takaku Y, Kurashima K, Ohta C, Ishiguro T, Kagiyama N, Yanagisawa T, Takayanagi How many instructions are required to correct inhalation errors in patients with asthma and chronic obstructive pulmonary disease? Respir Med. 2017 Feb;123:110-115. doi:
10.1016/j.rmed.2016.12.012
- Inhaler Error Steering Committee; Price D, Bosnic-Anticevich S, Briggs A, Chrystyn H, Rand C, Scheuch G, Bousquet Inhaler competence in asthma: common errors, barriers to use and recommended solutions. Respir Med. 2013 Jan;107(1):37-46. doi:
10.1016/j.rmed.2012.09.017
- Czobor P, Skolnick The secrets of a successful clinical trial: compliance, compliance, and compliance. Mol Interv. 2011 Apr;11(2):107-10. doi: 10.1124/mi.11.2.8
- Observational study to assess inhalation and handling errors of pocket inhalers for the treatment of respiratory diseases, before and after using the inhalation trainer of the Kata app – Statistical Report, 2021; Combined Usability results 2020/2021